
BPC-157
dangerous

TL;DR
BPC-157 likely works as a healing agent, but it might cause anhedonia and cancer. Whether it should be taken depends on the situation at hand. In terms of what parts of the body the drug acts on, perhaps the better question to ask which ones it does not heal — there are studies that find positive effects on joint, muscle, and even gut recovery.
Low doses (0.1-123mcg/day) are likely sufficient for humans; the conventional doses (200-1000mcg per day) that are recommended online are much higher than the ones used in animals, controlling for body weight. Multi-day dosing could potentially increase the drug’s potency.
About 20% of people on reddit who took BPC-157 report anhedonia — the inability to feel pleasure or pain — as a side effect. It’s possible that BPC-157 interacts with catecholaminergics (SSRIs/NDRIs/etc), and counteracts their effects, potentially inducing anhedonia or withdrawal. I took it while on adderall, and that might have factored into the anhedonia I got from it. I quit, and it went away. (Edit: I started taking it again in the form of 1mg of KLOW/day for a week, and I didn’t experience the anhedonia again).
Most people report the side effect being temporary; a few say it was permanent.
The science
BPC-157 is a peptide that acts as a broad-spectrum healing agent. It can be taken orally or injected into the body; it’s considered to effectively repair ligaments, muscles, bones, skin, the gut, and much more. We don’t know how BPC-157 works. Most of the theories (e.g. VEGF activation, NO-1 modulation), involve the compound activating receptors that lead to the the body spending more resources on healing itself. We don’t know if the body even makes BPC-157; the peptide itself is derived from a protein found in gastric juice — which doesn’t leave the digestive system.
Human studies on the compound itself are bad, typically containing no control group or an extremely small number of subjects. Dosages, drug interactions, effect sizes, and side effects have not been documented. Typically the recommendation online is to take 200-1000mcg of BPC-157 daily, cycled for 4-8 weeks, then 2-4 weeks off. Quite a large dose compared to what the animal literature uses.
There’s several justifications that one could make for that dose. If there is a dose-response relationship between the peptide and its effect, then it would be ideal to take a higher dose. It’s possible the pharmacokinetics of the drug differ significantly between humans and animals, making it so humans require larger doses for comparable effects.
These are not bad ideas; the recommended doses are still absurdly high.
Let me pull up a few rat studies. In this one, doses as low as 10ng/kg — 0.7 mcg in humans — are as effective as doses of 10 mcg/kg. That’s a 1000x difference.
The context here is that they disconnected the muscle and bone in the quadriceps of some rats. Apparently, an injury that does not heal on its own in their species; adding BPC-157 to their water reattached the muscle to the bone.

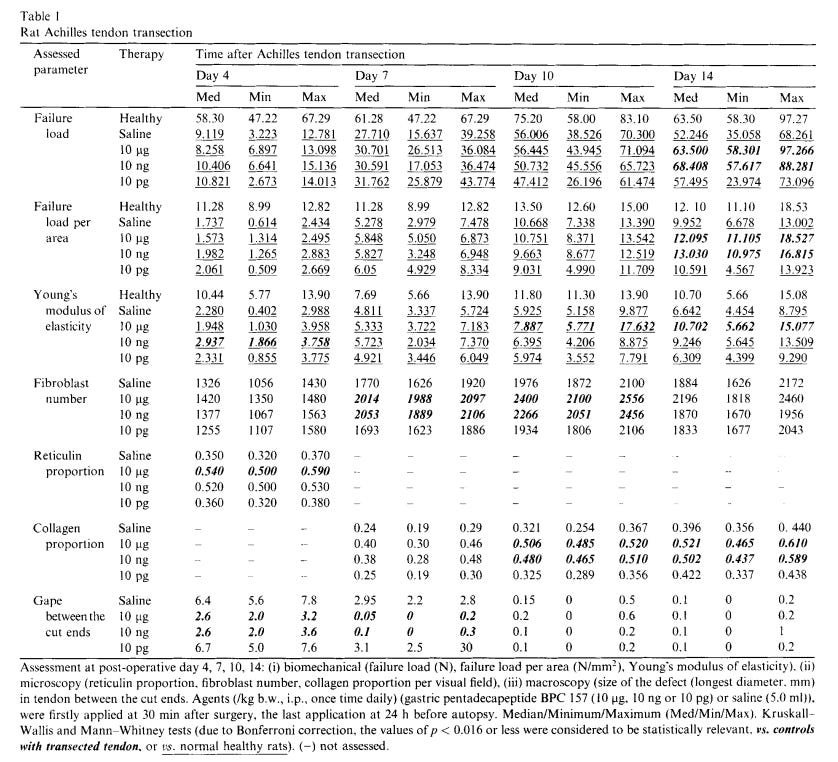
A different study on healing severed achilles tendons in rats found something similar, though the rats in the control group also healed eventually. It sped up the healing process by about 10-20%, in all doses except for 10 pg/kg, which was completely ineffective.
BPC-157 research is infamously concentrated in a Croatian research group led by Sikiric, the developer of the drug. A boring criticism; there are also studies conducted by people outside that circle that also find positive results.
A Korean study administered some rats a single injection of saline, BPC-157, or morphine. 60 minutes later, they either injected them with formalin (toxin) or made a small cut to their hind paws — a 2x3 study design. They sowed up the incisions and treated with anti-biotics. They then monitored their responses to pain over the next seven days.
Rats treated with BPC-157 had more blunted responses to pain, indicating either a better recovery or an anesthetic effect. Rats treated with morphine fared better after it was administered, then worsened, probably because of withdrawal.

In the formalin test, rats treated with BPC-157 flinched less than those administered with saline 10 minutes after the formalin was injected; but not 10-60 minutes later (in phase 2).
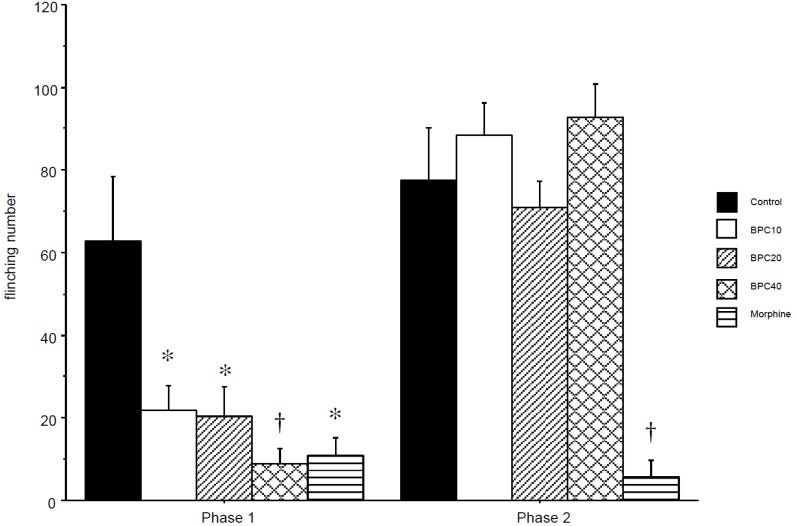
There existence of a dose-response effect here looks quite ambiguous, despite the statements of the authors. It also might be the case that the dose-response effect differs between effects — the anesthetic and therapeutic ones — assuming they exist in the first place. The doses of BPC-157 used here are also quite high, above when you would even expect the dose-response effect to appear.
It’s pretty clear BPC-157 works in animals, it would be overkill to go through more studies. There is still the question of human extrapolation, whether doses in rats generalise to people.
Typically, humans are given lower doses of drugs than rats are, due to their lower relative surface area and slower metabolism. The FDA’s heuristic is that, for coverting rat/mouse drug doses to humans, the amount must be 6.2-12.5x lower controlling for body weight. This is not necessarily the case for BPC-157, but there is no particular reason to think that it does not.
In rats, the bioavailability of BPC-157 is 14-19%; within beagle dogs it’s 45-51%. Rats are more genetically similar to humans than dogs; regression-to-the-mean logic implies it’s likely that the human bioavailability is higher than the rat one. Unless BPC-157’s effects within humans differ significantly from those observed in rats and mice, it’s possible that doses as small as 0.1 mcg1 are effective in humans.
Which is insane, and likely wrong, but keep in mind that BPC-157 is a compound that activates receptors. It’s unlikely it does the dirty work of repairing the body itself.
My intuition is that the rate limiting factor in the efficacy of BPC-157 is the volume of injected liquid, not dosage. At the 0.01-0.05ml range, it becomes more difficult to reliably control the volume due to various factors: dead space in the syringe, the precision of human muscles, and slanting (e.g. one part of the liquid being on the 4 unit bar, and the other part being on the 2 unit bar).
Most BPC-157 vials have a volume of 3ml and 5-10mg of peptide powder. This means that, realistically speaking, the smallest consistently injectable dose of BPC-157 is somewhere between 30-100mcg depending on the vial and syringe. Unless the solution is deliberately diluted by removing reconstituted peptide and replacing it with BAC water.
Ignoring the constraints of injecting, I’m not really sure what the optimal dose is. If we assume a worst case scenario: the human bioavailability is 10x lower than in rats, the surface area conversion factor doesn’t apply, and maybe humans even have some unique quality that makes the drug 10x less effective — that gives us a worst-case dosage of 62-123mcg2. Still much lower than what people tend to use.
My intuition regarding the dose-response effect is that injecting more is not better. Even when people have severe and urgent injuries like gunshot wounds, there is little the body can do to speed up the recovery process. Even with all the drugs, energy, and water in the world. Releasing more healing signalling molecules should theoretically redirect more resources towards the injury, but the thing is that it seems the signalling can only do so much. Gunshot wounds take at least several weeks to heal, even with state of the art medical care and optimal health.
There is also the question of dosage frequency. People typically recommend daily doses + cycling the drug. I don’t think this is necessarily ineffective, but the drug clears from the body pretty quickly; the half life is lower than 30 minutes… in rats and dogs. People who want stronger effects might find better results from dosing 3 times a day rather than 3x as much at once.
Cancer
BPC-157 is a generally well-tolerated drug. Humans taking it report few side effects, and neither do studies on animals. A lethal dose has not been established.
One of the major concerns with the drug is that it causes cancer. BPC-157 is an angiogenic drug, which means that it contributes to the formation of new blood vessels. Theoretically, these could latch on to new tumours and contribute to their growth — causing cancer.
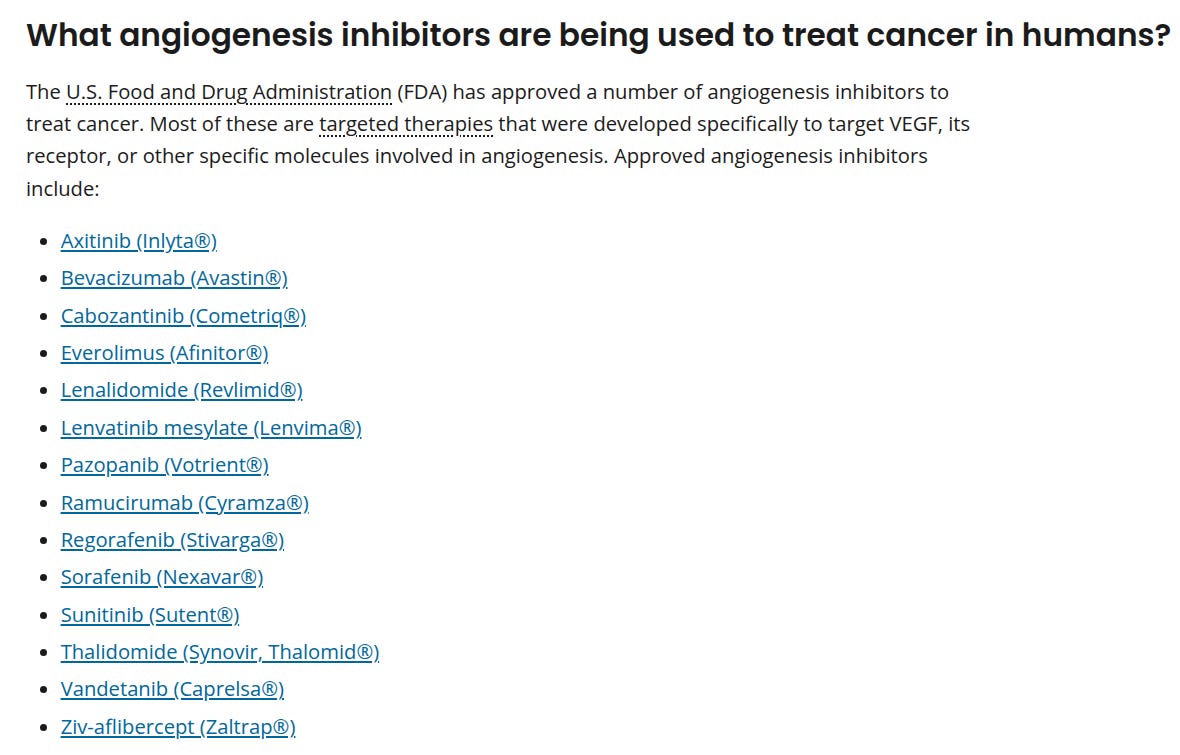
Some anti-cancer drugs, like Axitinib, treat cancer by doing the exact opposite of what these peptides do: inhibit angiogenesis through the VEGFR pathway (however that works). Many other cancer treatments are angiogenic inhibitors, for that matter.
Things that have been proven to cause cancer in humans are almost always shown to be carcinogens in animals. So much, that some scientists think that all human carcinogens also cause cancer in animals. I’ve heard some say that arsenic causes cancer in humans but not animals, but that’s it. That said, there is no evidence (not saying bad evidence!) BPC-157 causes cancer in animals. It’s all theoretical.
No evidence does not mean an absence of effect here; testing for carcinogenic effects properly requires a specialised methodology due to the fact most animals have shorter lifespans. In some cases, animals (e.g. mice) genetically altered to have cancer mutations or the implantation of tumours into animals to see if the cancer grows.
Some people have claimed that BPC-157 is an anti-cancer drug. That’s not necessarily false, but there is no good empirical evidence to support that claim:
The comment by Sikiric et al. cites “anti-tumor potential” yet offers no published in vivo tumor-growth or metastasis studies. A single melanoma cell-line experiment from 2004 [8] (unreplicated) is insufficient to support anticancer claims, while pro-angiogenic signaling remains a plausible tumor-promoting hazard. To date, no published in vivo data demonstrate that BPC 157 inhibits tumor progression, reduces tumor volume, or suppresses metastasis.
In line with this, in the comment, the authors claim that oncologic risks are “entirely excluded,” yet they fail to cite a single in vivo study involving solid tumors. Paradoxically, their own previous work demonstrates BPC 157 activates angiogenic signaling—precisely the kind of mechanism known in oncology to potentially support tumor growth. The study by Kang et al. [9], which was cited by the group of Sikirc et al. as a solid confirmation of in vivo anti-tumor activity mediated by BPC peptide, primarily focused on alleviating symptoms of cachexia and inflammation in tumor-bearing animals, rather than inhibiting tumor growth or destroying cancer cells. Therefore, such studies cannot be interpreted as the evidence of BPC 157’s antitumor activity but rather as a potential supportive effect on the overall condition of the diseased organism.
I’d say it’s likely BPC-157 causes cancer; we don’t have the proof it does yet.
Anhedonia
Imagine if there was a drug that turned you into the king of the world, but removed your ability to feel anything. Would you take it? I assume not.
The argument about BPC-157 potentially causing cancer dominates scientific discourse, but people who actually take the drug seem to be complaining more about anhedonia. Particularly, when they take it with certain medications; the common link I see between them is that they are catecholaminergics: adderall, SSRIs, and whatnot.
The “experts” claim that there is “no evidence” that BPC-157 causes anhedonia. Of course there is no scientific evidence it does. Where are the human studies?
I took BPC-157 for about a week, in the form of KLOW: a combination of GHK-cu, BPC-157, TB-500, and KPV. Took it because of struggles with chronic knee pain + a subluxated shoulder. Tried various doses out of curiosity — 66mcg, 132mcg, and 625 mcg (intramuscular, into deltoid). Didn’t notice any differences in effects.
Felt great on it, regardless of the dose. Nasal passage was clearer, pain/fatigue improved, and it was just easier to move my body. The shoulder seemed to start recovering faster, but it’s hard to tell because of the way recovery works.
Unfortunately, I felt anhedonic. I quit. I recovered within a week.
I was also taking adderall at the same time. I quit that too, as a precaution.
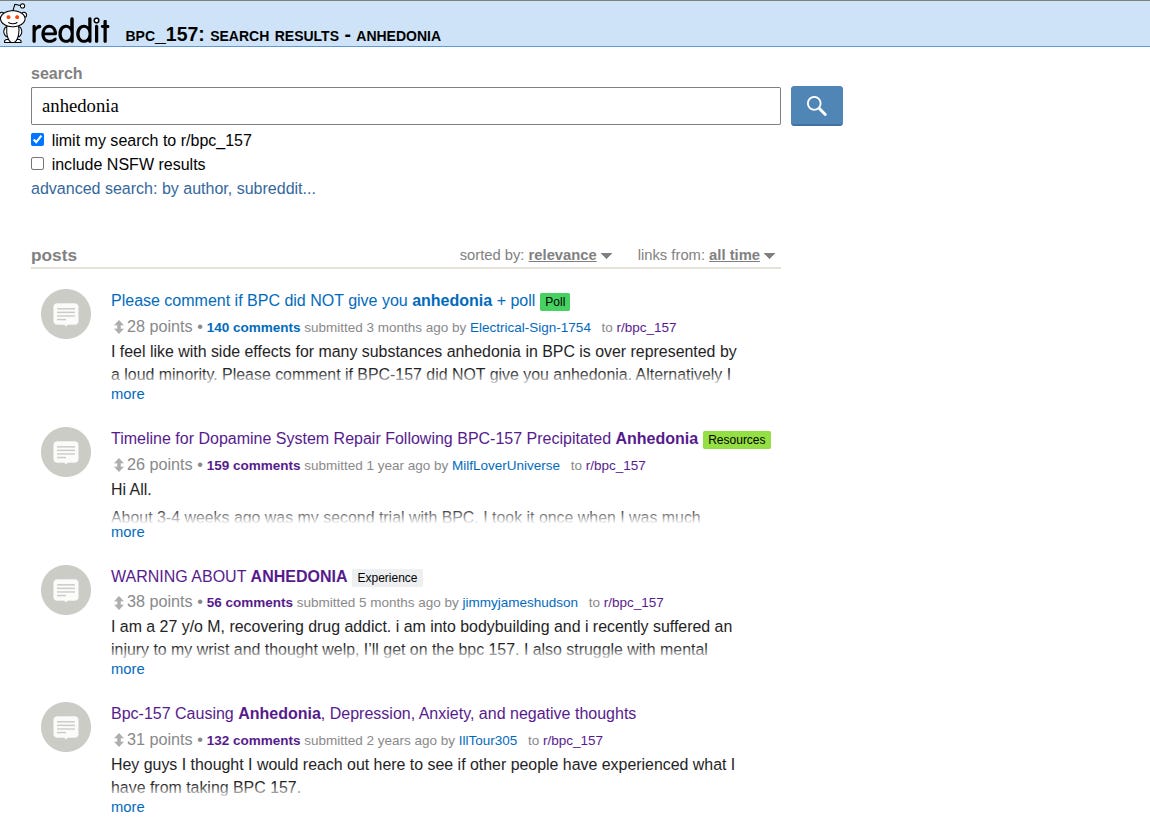
Many such cases. Somebody asked about said side effect on reddit, and people commented on whether they got it. 17 said yes, 58 said no; 9 were complicated cases.

That means 20% of people in the thread who took BPC-157 reported anhedonia. A large number; you’d struggle to find a figure that high, even for something like SSRIs.
Apparently for some people, the anhedonia is permanent (!). One of the worst side effects you could get from any drug. Even worse than getting cancer — at least you can still enjoy life.
Generally, I’m pretty skeptical of cases like these. It could be an attribution error, where the permanent side effect was caused by something else. It could be psychosomatic: people getting in their own heads about whether they are experiencing something so much that they actually experience it. That doesn’t mean the drug didn’t cause anhedonia; it just did it through a different causal pathway.
Here’s the problem. Now you know you could get anhedonia from taking BPC-157. So if you take it, you will monitor your body to check if it happens to you. The problem is that a lot of things that are enjoyable are that way because you aren’t checking yourself. You become absorbed. Asking yourself whether you like a video game pulls you out of the trance, and makes the magic disappear. But if you don’t check yourself, you could be wrecking yourself. Quite the catch 22.
When I was on BPC-157, sometimes I would just stare at a computer screen, wanting to care about something, but I couldn’t. I was worried about whether I permanently damaged, and didn’t even feel any dread about what I did. I just felt empty.
I checked out some of the animal studies on how BPC-157 interacts with amphetamines and hedonic responses. It seems that BPC-157 counteracts some of the effects of amphetamines on rats, including repetitive behaviour; it also seems to heal disruptions in behaviour caused by chronic amphetamine use.
So maybe the anhedonia wasn’t caused by BPC-157 itself, but by nullifying the effects of adderall, which then sent me into withdrawal — which caused the anhedonia.
I am not here to give medical advice — I do not have a medical license — but if you also have chronic pain caused by joint hypermobility, it’s unlikely that BPC-157 or anything in KLOW will fix it. It may do so temporarily, but it would be unwise to take a drug that may cause cancer for your whole life, even if it is cycled.
BPC-157 Adverse Event Database
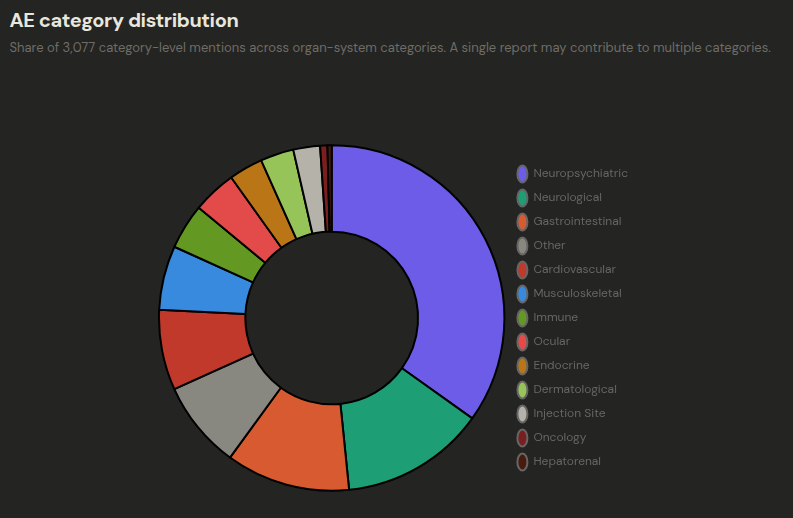
Anthonystaj has developed an adverse event database for BPC-157 by mining every single reddit thread that mentioned the drug. In total, 1370 users reported 4254 side effects. Half of them were neurological:
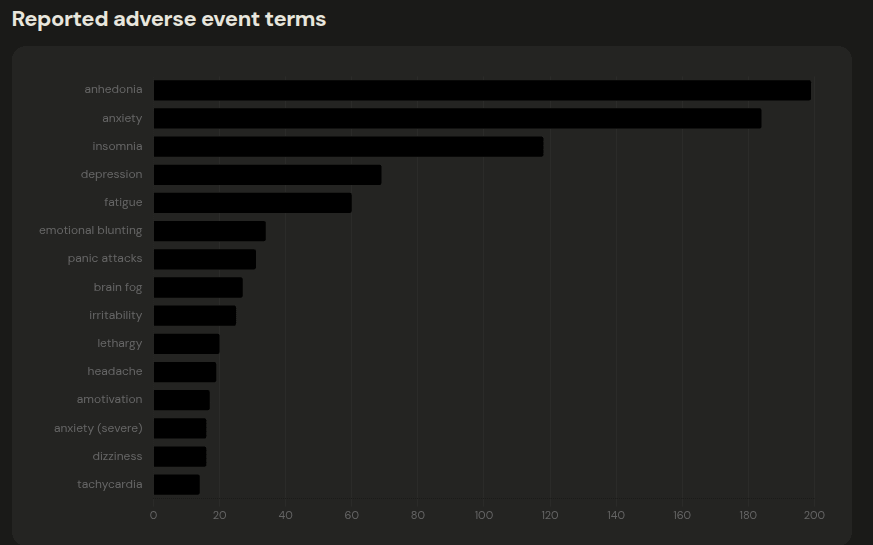
Anhedonia was at the top of the list, when it came to psychiatric side effects:
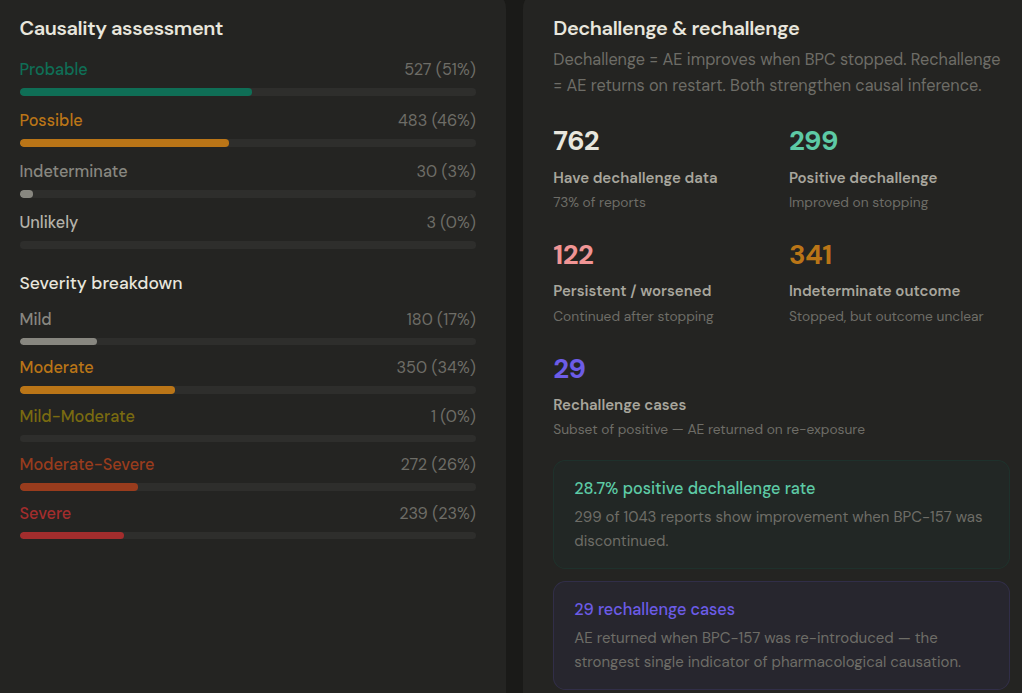
Of these neurological cases, 29 showed rechallenge data: the side effect came back with use:
The legal question
I think BPC-157, and all peptides like it, should be legalised anyway. No matter how dangerous. Logic is simple: before legalisation, main and side effects can’t be proven the same way. If it’s legalised, and it’s dangerous, the danger will show up in the data. Then we can make them illegal. That is the meaning of accelerationism.
min effective dose in animal studies = 10ng/kg — convert to 70kg human — 0.7 mcg. Add the surface area conversion (6.2 in rats; 12.3 in mice), and you have ~0.1 mcg.
0.1 mcg x 10 (hypothesised lower bioavail) x 6.2 or 12.3 (rat and mouse conv factor) x 10 (hypothesised magic characteristic) = 62 - 123 mcg
Is this a common side effect in medicine as a whole? iirc martin shkreli's take was that the high molecular weight of peptides like BPC-157 would both reduce efficacy but also be safer than most small molecule medicine because its harder for it to cross lipid membranes or the blood brain barrier. I think it could just be a nocebo effect
Tour de force write up, kudos for pulling all that together, and even doing a sizing of anhedonia side effects triangulation.
One of the most interesting parts to me, that I hadn't previously been aware of, was your section on rat / mice dosage adjustment. I'd always wondered why the longevity people thought they could get away with ~10x lower doses once per week of Rapamycin vs the mouse studies, and that answered it directly.