
What is Ehlers Danlos syndrome?
and does it exist?

Ever since I was a child, I’ve had extremely flexible joints and strechy skin.

What was initially an inside joke at school took a turn for the worst. Around the age of 15, I started weightlifting, and ended up injuring my elbows and knees. To the point that it hurt to walk, so I limped instead. I even used crutches a few times.
I wasn’t sure what was the problem. Maybe I was lifting too often, or with poor form… which was probably true.
The exact chain of events is blurry, but at some point, I started to connect the dots between flexible joints and joint pain. It’s a common complaint of patients with hypermobile joint disorders — flexible joints tend to overextend and get injured, and are less capable of sustaining weight.
So my mother drove me to the hospital to see a doctor. I told him that my joints were in pain, and that I thought it was connected to the flexibility of my own joints. He was pretty convinced of the flexibility after a demonstration. The doctor, unfortunately, said there was nothing he could about the pain, that there was no cure for my condition.
I stopped listening after he said that. Later, my mom told me that he thought I did have some kind of hypermobility disorder. I haven’t bothered seeing a doctor about the issue since.
II.
Ehlers-Danlos syndrome (EDS) refers to 13 different connective tissue disorders, unified by joint hypermobility and strechy skin. Lesser-known complications incude cardiovascular failure, joint pain, and scoliosis. Some people with the disorder do not have the characteristic strechy skin. Treatments are limited in variety and efficacy — typically losing weight and strength training are encuraged; sometimes opioids are prescribed for pain, but doctors are generally wary of doing that. The disorder itself is genetic and incurable.
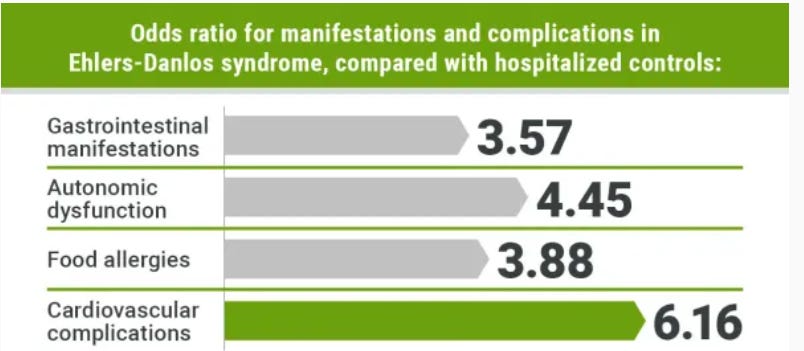
It also turns out that Ehlers Danlos syndrome is correlated with a variety of symptoms and medical conditions: narcolepsy, POTS, ADHD, autism, LGBT identification, MCAS, allergies, IBS, and dysautonomia. That covers, well, everything in the body — the brain, sex, cardiovascular system, gastrointestinal system, immune system, and nervous system.
Some of the effect sizes are large: 42.5% of EDS patients have a psychiatric diagnosis — the condition is most strongly associated with autism (7.4x) of all mental disorders. Transgenders are 132x (?) more likely to have a hypermobile joint disorder. Which replicates too — a different study found 17% of teenagers with EDS are trans.
Personally, I’m inclined to believe some of these associations are real. I have some of these comorbidities1, and so do my siblings. They also have flexible joints, but not to the same extreme. You could say they regressed to the mean.
It would also be surprising if mutations affecting collagen, the most common protein in the body, were specific to just joints and skin. It’s also found in the brain, gut, teeth, cornea, and spine. Name a random body part: it’s more likely than not that collagen is there.
There is a theory the correlations might be specific to clinical samples due to selection, but it’s hard to test that theory, since EDS is such a rare disorder. This has caused people to say there is “no evidence” EDS is associated with these conditions.
Bad evidence is bad, but it is still evidence.
Related: The Phrase “No Evidence” Is A Red Flag For Bad Science Communication
The critics of the comorbidity literature are essentially arguing that the symptoms of connective tissue disorders are limited to the skin and joints, even though there is connective tissue everywhere in the body. Which is a ridiculous null hypothesis. It’s not even a good alternative hypothesis.
III.
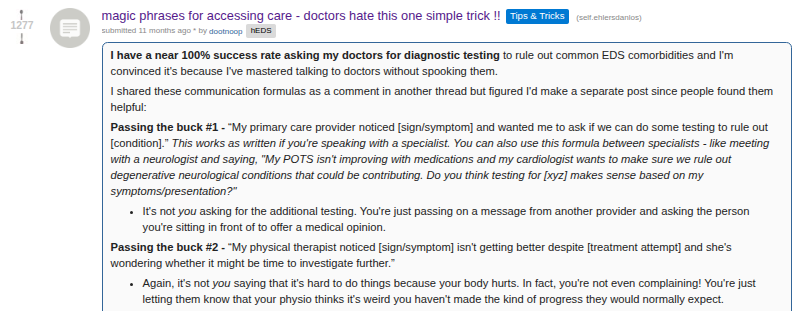
On reddit, people with hypermobility disorders report being ignored, belittled, or rejected by their doctors for seeking care. The r/ehlersdanlos subreddit even has posts that advise people on how to work with doctors to get medical testing:
70% of people diagnosed with a joint hypermobility disorder are women; about 95% (?) of the people seeking care for it are female. It’s an autosomically-caused disorder, so the true ratio is 50/50, but sex differences in musculature and the formation of connective tissue lead to the disorder having an exaggerated expression in women.
There’s another variable at play. I assume a lot of the other men with joint hypermobility did what I did: went to the hospital, got told the condition isn’t curable, and left. Women, on the other hand, are more likely to seek diagnoses and care for medical conditions in general.
The male strategy is definitely more culturally valorised. Is it better? Not really. Sometimes, not seeking medical care for uncertain or benign symptoms works: the symptom either doesn’t matter or it goes away on its own. Other times, it leads to late diagnoses or symptoms not getting proper treatment.
Ehlers Danlos Syndrome has acquired a reputation for being an “instagrammable illness”, one that people fake or aesthetise for attention. This has been invoked as an explanation for why hypermobile joint disorders have so many comorbidities.
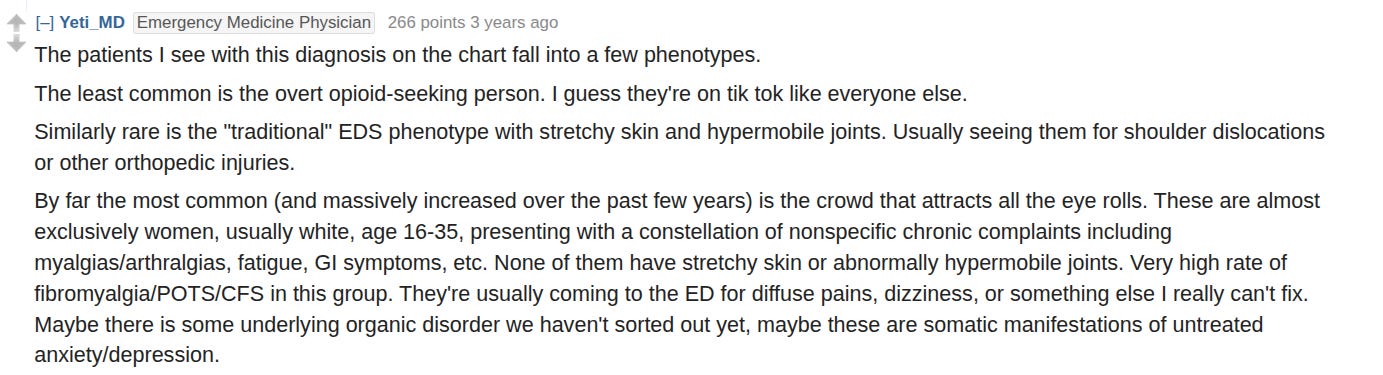
The diagnostic environment for people with EDS is already complicated. Then you add in the instagrammable ilness stigma, which makes doctors suspicious of people seeking care for the condition, maybe for good reason.
These debates about the social dynamics of EDS bore me. Muddled by Judeochristian2 morals and idiots on the internet. Let’s pull out the economics.
A patient has physiological problems — pain or fatigue — perhaps caused by joint hypermobility. Incentives pull them away from the medical system because it does not reliably diagnose the condition or provide options for treatment. So people pivot to the internet to get what doctors normally give them: validation, information, and suggestions for treatment.
But it’s still the internet: full of hypochondriacs, grifters, false information, questionable anecdotes, and people who just want attention. That then affects the reputation of the disorder, which makes its diagnosis more difficult.

The fact that EDS is incurable, rare, and illegible enables people to fake it. So they do. Not much more depth to it than that.
In other words, Ehlers Danlos syndrome being a meme is downstream of economic incentives and the biological constraints of the disorder. Not random social trends, or evil people in a room full of smoke.
IV.
Oh, and I forgot to say. Ehlers Danlos Syndrome is a made up disorder.

Worse, it’s not even good at being a made up disorder.
It’s more analogous to ‘intellectual disability’, than something concrete like Down’s syndrome — except that it affects connective tissue and not the brain.
There is no consistency in what is and is not ‘Ehlers Danlos Syndrome’. If it was mutations in collagenous genes, then Alport syndrome would qualify. It’s not hypermobility: there are genetic disorders associated with hypermobility that do not form part of the EDS umbrella (e.g. Marfan syndrome). There are even types of EDS, like Musculocontractural EDS (mcEDS), that are associated with stiffer joints.
Maybe Ehlers Danlos syndrome is supposed to be an umbrella term for joint hypermobility disorders with specific causes that generalise past skin and joints — like brittle cornea syndrome. Using the intelligence analogy — joint hypermobility is analogous to having a low IQ, independent of whether there is a specific cause, like brain trauma or a chromosome deletion. Ehlers Danlos is more like Down Syndrome: not only do people with Down’s have a low IQ, but there is a specific cause (trisomy) and accompanying comorbidities, like obesity or a short neck.
This would make sense… if there wasn’t another vague diagnostic label under the EDS umbrella — hEDS. A joint hypermobility disorder with an unknown cause. Translated into English, it means “there’s something wrong with your connective tissue and we have no idea what it is”. And that still ignores the many disorders that feature joint hypermobility that are not categorised as subtypes of Ehlers Danlos syndrome.
A different way to see it: there are 28 different types of collagen. Coded by 44 genes and 2 pseudogenes. In total3, those genes add up to about 6,567,598 base pairs. Assuming ~95% of mutations are benign, that gives us 300,000 potentially causal variants — most of these will not vary in the general population, and if they do, only a few will have large effects. And then you have all of the genes that affect connective tissue that have nothing to do with collagen.
If so many genetic mutations and variants could affect the expression of connective tissue, the reasoning behind grouping a bunch of disorders under one label starts to look a little unreasonable.
‘Syndromic intellectual disability’ is a useful label, because it gestures at a problem (low IQ) and the suspicion of a single cause, without having to identify one. ‘Ehlers Danlos syndrome’ is not, because it is pretending to identify a specific cause without actually doing it. And everybody loses their minds: patients, doctors, medical researchers, and people on reddit.
V.
The beighton score is the IQ test of joint hypermobility. It involves testing whether the thumbs, elbows, knees, and spine can bend past a certain point, and adding up the nine tests into one score.

An OK idea which… somehow turned into the gold standard hypermobility test.
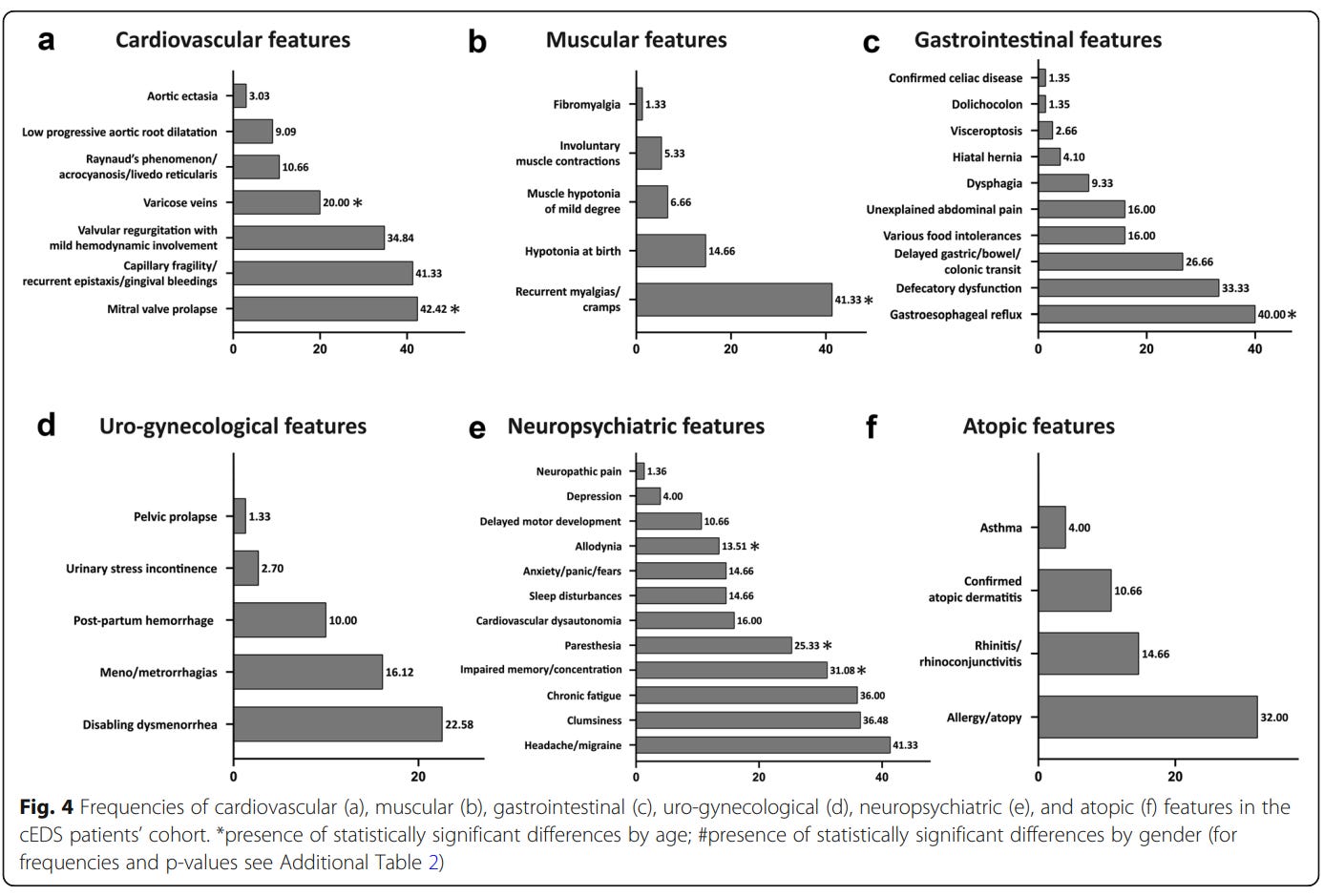
The biggest problem is that the expression of even a single type of Ehlers Danlos syndrome varies significantly. Among people with genetically confirmed cEDS, which supposedly causes generalised joint hypermobility, only 59% pass the beighton test:
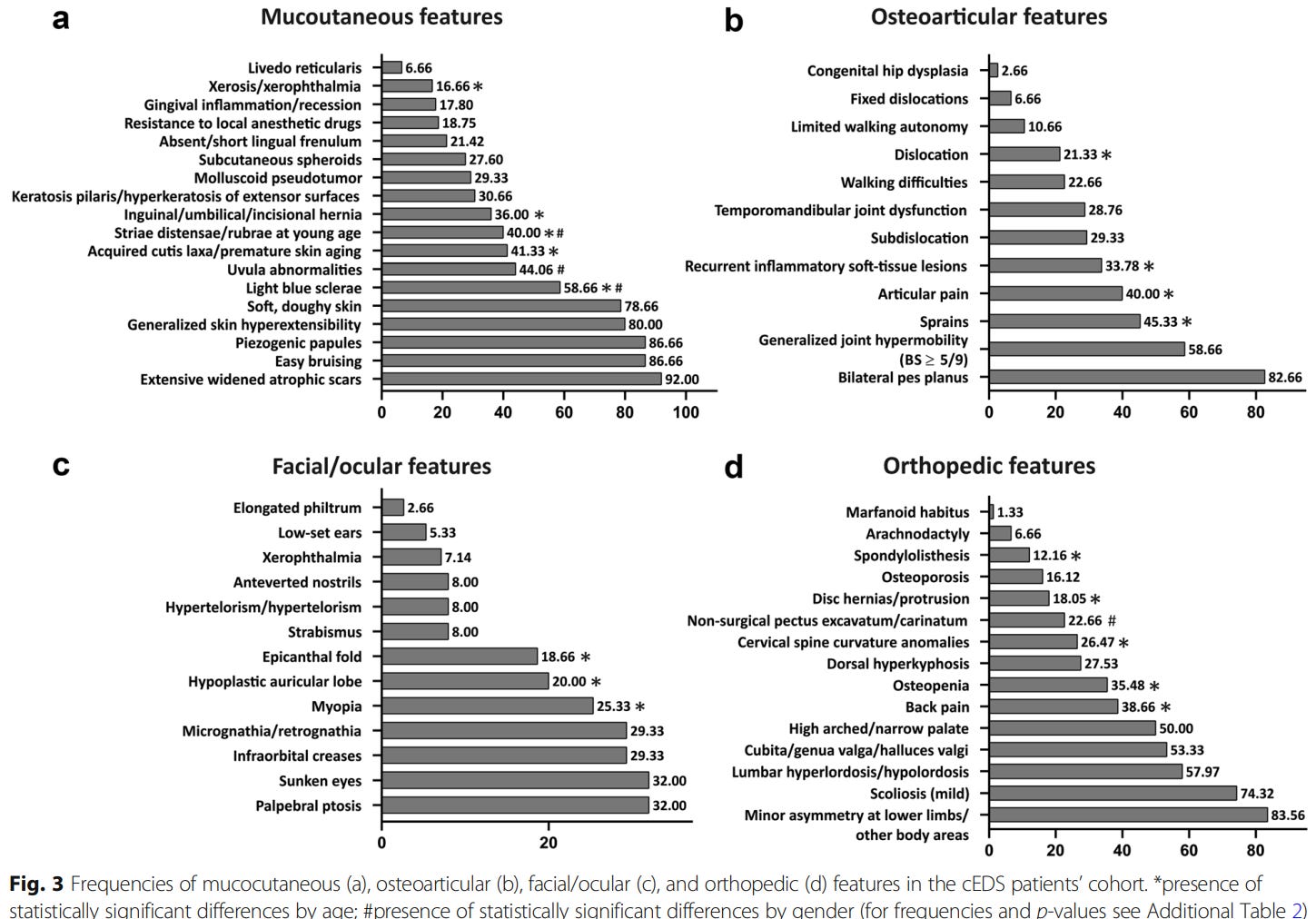
They also reported the frequency of comorbidities. Based on a visual glance, they seem high, but not as high as the percentages in the comorbidity studies.
What’s the problem?
Circling back to the intelligence analogy, there is a consensus that an IQ test alone is awful at diagnosing intellectual disability. Not just among the people who are labelled as experts, but among the IQ-realist crowd as well.
Why? Well, it simply doesn’t work.
Let’s use 22q11.2 deletion syndrome (DiGeorge syndrome) as an example. In accordance with its name, it involves a deletion in part of the 22nd chromosome, which causes intellectual disability and some other comorbidites. These individuals score about 2 standard deviations below the average person on an IQ test.

The myth on the internet is that an IQ score of below 70 equals mental disability. If 70 was the cutoff, only half of the people who have the mutation would get diagnosed, and about 2% of the general population would be shoved into the same category; most of who do not have any specific problem, besides scoring poorly on a test.
Now, we circle back to Ehlers Danlos syndrome (this will happen many times). The reliability of the beighton test is mediocre — a meta-analysis of 24 studies found a mean inter-rater reliability of 0.75 — the authors of the publication thought that implied the beighton scale was a “highly reliable clinical tool”. An offensively incorrect interpretation4, which can be ignored for now.
When we are diagnosing people with Ehlers Danlos syndrome or another hypermobility disorder, we are dealing with outliers. Typically, outliers regress to the mean in a disproportionate way — this is called the winner’s curse in statistics.
This phenomenon makes it difficult to identify gifted students with IQ tests.
When using composite ITBS scores, which have a reliability of 0.98 (??): 50% of students who were labelled as gifted in 3rd grade would not have qualified as such, had they been tested in the 8th grade instead.
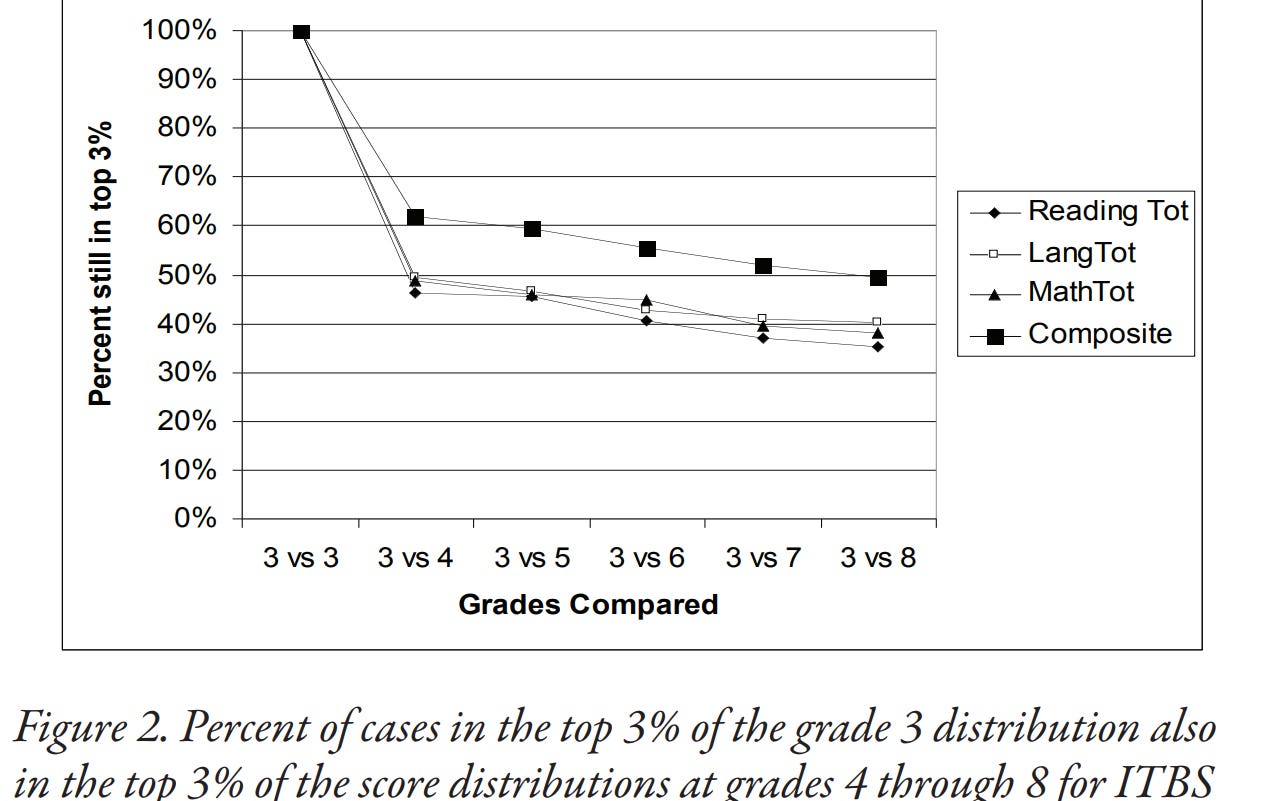
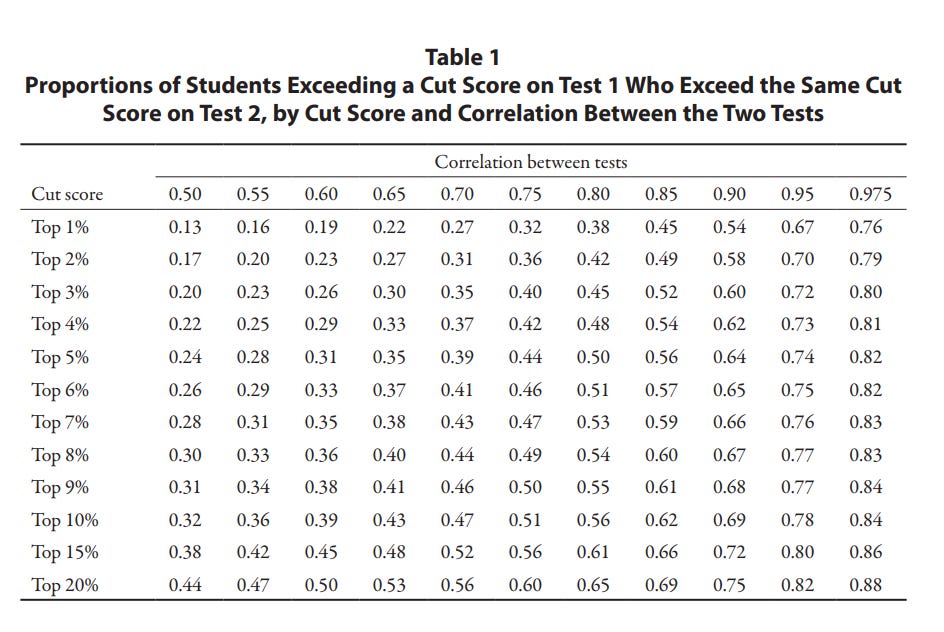
Part of this is that people have different developmental curves for intelligence, but it also has to do with the way cutoffs work. A test with a reliability of 0.9 will still misclassify 50% of the people who scored in the top 1%.
Doctors using beighton scores to diagnose Ehlers Danlos Syndrome are doing something far more ineffective: using a tool with a inter-rater (aka maximum) reliability of 0.75, to diagnose a disorder with a rarity of 1/5000.
My argument here isn’t that a lot of people are incorrectly diagnosed with hypermobility disorders by fluking the beighton, though I’m sure that happens. It’s that many people, particularly with forms of EDS that do not cause generalized hypermobility, are being screwed over by a simplistic and mediocre test.
In some cases, these missed diagnoses can make the difference between life and death. Vascular EDS in particular can lead to random arterial ruptures, which can be fatal; the life expectancy of people with the condition is about 50 years.
VI.
Medicine and psychiatry both have a problem where they want to merge classificatory and diagnostic labels. ‘EDS’ is a classification. ‘A mutation in the COL5A1 gene causing strechy skin and hypermobile joints’ is a diagnosis.
This also generalises to other debates in science — is chronic fatigue real? As a symptom, sure. As a disorder — chronic fatigue syndrome? The wrong question. If we can identify a causal pathway by which people have persistent fatigue, then why don’t we call that its own thing?
Then we have psychiatry. Is ADHD real? Or is it another way of reframing low conscientiousness/intelligence/energy/executive function, a personality type, or disliking rejection, spreadsheets, and school? Arguing ADHD is one of these things is kind of like answering the question “what do you want to be when you grow up?” with a colour. “I want to be red when I grow up” — “ADHD is executive dysfunction”.
ADHD is a classification used to identify problems that can be solved with stimulants.
There is an uncontested assumption in the EDS discourse that I have not seen other people highlight — whether knowing you have the disorder matters. Does knowing you have an uncurable, rare disorder actually help you? Making you feel special doesn’t count.
My vote is yes.
Let’s say God swoops down from the heavens to tell me my recurring joint pain is not caused by hypermobility.
Well, my joints are still in pain. What causes that then?
Maybe the pain is psychosomatic. Does knowing that matter? To me, it does.
What if the pain is caused by a different disorder, like rheumatoid arthritis? Well, that can actually be treated.
VII.
To have Ehlers Danlos Syndrome is to have a body that does not work, because of a disorder that does not exist. You can try going to a doctor — most of them will not know about the disorder. If they do, they might just assume you are malignering (aka a munchausen) from the get go. And if they do trust you, they are likely to use inadequate diagnostic methods like the Beighton score. And then, even with a diagnosis, there is little the doctor can do to help you, even if they care. Internet communities can give some useful information… but it’s still the internet. The truth of whether you have this nonexistent disorder will still matter to you, even if nobody understands why.
And that’s if you are lucky enough to live a developed country.
Narcolepsy: probably. I have the sleepiness, hypnohallucinations, and disordered sleep. The condition accelerated around the ages of 16-20. Some symptoms, like sleepwalking and randomly falling into deep sleep, were there since I was young.
ADHD: subclinical. Older sister, younger sister, mom, and all three of her siblings have it. Yes, all four.
Autism: subclinical. The only psychiatrist I ever went to thought I had aspergers, but my mom pushed back against the diagnosis; it would have prevented me from going to private school (didn’t grow up in the US).
Depression, anxiety, headaches: fortunately not.
Allergies: cats, dogs, and probably pollen. Went into anaphylactic shock after chewing on a Brazil nut… it was so disgusting I spit it out and washed out my mouth. Some nuts really are too bitter to swallow. Dad (not hypermobile) and older sister also have problems with allergies. Thankfully, H1-blockers are highly effective and OTC.
POTS: maybe. Ever since I was a child, I would occasionally see stars whenever I stood up. I thought that was normal, but it indicates a drop in blood pressure. My blood pressure off stimulants (~95/55) is very low. I’ve randomly fainted twice already. Sister was diagnosed with the condition; brother also faints a lot, but I don’t think he’s talked to a doctor about it.
Tinnitus: when I was a child, I thought it was normal to hear buzzing in quiet environments. Apparently that’s, well, tinnitus. Not bothersome or particularly elevated though.
Temporomandibular Joint Disorder: if I open my jaw far enough I hear some popping sounds. Not bothersome or notable. It’s also common in Latin Americans.
Subluxations: they come and go. Just had a shoulder sublixation like three weeks ago.
Wrist pain: used to have issues with it. I honestly think it was psychosomatic. My joint hypermobility is nonexistent in smaller joints; other people have reported similar experiences with gaming causing psychosomatic joint pain. Specifically, Mikyx (LoL player) reported having problems with wrist pain, which improved after reading a book about… back pain. From what I read, it identified the autonomic nervous system as being implicated in chronic pain. Don’t know if that’s actually true. My impression is that the author is saying “psychosomatic conditions cause chronic pain” in a scientific and emotionally acceptable way.
IBS: used to have it. Changed diet. Went away. Don’t even remember what I changed, but I’m glad it’s gone. Maybe I shouldn’t ask too many questions…
I noticed my right ring finger was deformed when I was 16 years old, and thought it was from playing video games or excessive computer use. Apparently, it’s called a swan neck deformity, a side effect observed in hypermobility disorders. Not sure if that is the actual cause though, since my small joints aren’t hypermobile.

I apologise for the horrible sins of my ancestors.
The math:
# A tibble: 44 × 4 geneSymbol n_transcripts genomic_length longest_transcript <chr> <int> <int> <dbl> 1 COL10A1 5 33409 3498 2 COL11A1 16 232050 7327 3 COL11A2 43 30070 6425 4 COL12A1 14 121728 11725 5 COL13A1 51 157239 3396 6 COL14A1 11 248472 8009 7 COL15A1 18 128094 5547 8 COL16A1 20 51767 5418 9 COL17A1 18 55183 6164 10 COL18A1 33 108598 6586 11 COL19A1 5 345913 8740 12 COL1A1 27 17531 5914 13 COL1A2 19 36408 5993 14 COL20A1 10 41621 8097 15 COL21A1 11 337505 4173 16 COL22A1 8 325807 6394 17 COL23A1 9 352776 2899 18 COL24A1 5 427540 6834 19 COL25A1 8 494028 8026 20 COL26A1 11 196623 3409 21 COL27A1 8 156975 7813 22 COL28A1 6 177999 4297 23 COL2A1 10 31723 5275 24 COL3A1 25 38374 5490 25 COL4A1 25 158240 6742 26 COL4A2 29 207398 6547 27 COL4A3 13 150169 8038 28 COL4A4 8 161492 9984 29 COL4A5 15 257803 6531 30 COL4A6 13 283866 6750 31 COL5A1 8 203041 8442 32 COL5A2 6 147965 6829 33 COL5A3 2 50944 6207 34 COL6A1 10 23294 4203 35 COL6A2 36 36130 3891 36 COL6A3 25 90387 10532 37 COL6A5 4 139329 9226 38 COL6A6 3 159866 8689 39 COL7A1 11 31257 9276 40 COL8A1 46 160752 5714 41 COL8A2 3 29984 4669 42 COL9A1 16 86959 4339 43 COL9A2 17 17138 2926 44 COL9A3 17 24151 2497 > sum(collagen_lengths$genomic_length) [1] 6567598
A reliability doesn’t magically become high when it crosses a certain threshold. Even if it did, the threshold definitely would not be 0.75. And that’s an INTER-RATER reliability. That describes the agreement between two different raters of the same test — it would be more appropriate to describe the test-retest reliability.
Perhaps your parents fed you the gum gum fruit and you dont remember
Your discussion of medicine and psychiatry of medicine and psychiatry conflating classificatory and diagnostic labels reminds me of a conversation I had recently with my uncle... my aunt and their son are both psychotic but have different diagnoses with my aunt technically only being diagnosed bipolar despite her tendencies to scream at poles for hours. My cousin is only diagnosed schizophrenic. Presumably both are caused by the same genetic markers but the cause is so little known. I suspect they are just applying many labels to the same underlying cause, with slightly different expressions. I imagine psychosis is particularly hard to study just because paranoia makes patients less likely to cooperate; my uncle commented on my aunt neglected to mention many things to her doctor. I have paranoid tendencies which most resemble what I've heard of Cluster A personality disorders, probably also caused by similar genetic markers. But when I did briefly see a therapist about it when I was 18, they wanted to diagnose me with things as diverse as autism (because I was socially awkward, because I didn't talk to people because I was convinced they would stab me), OCD, depression, anxiety and schizophrenia. She was convinced I would devolve into a schizophrenic unless I took antipsychotics (which I read up on, convincing me not to take them). I ultimately became largely functional even though some of those tendencies remain.